 Text
Text 

Nigel Dupree, Project Director – Digital (Eye) Health, Accessibility, Literacy, Diversity & Inclusion Campaign.


The other Public Health Global Pandemic in Binocular Vision Loss
S.M.A.R.T. Foundation’s ethos has been modelled on the work of Carl Rogers, the American Psychologist who believed that all humans have the will to self-actualise – to fulfil their highest potential.
Since its inception, the Foundation has unconditionally accepted children and adults, allowing them to discover themselves, having fallen or been pushed through the educational gaps – fostering the time and space for them to self-actualise.
The children, young people and adults, who were considered ‘no hopers’ by the educational, social care and youth custody systems, seemed to thrive on unconditional positive regard, promoted by providing them with a ‘peer approved environment’ along with exposing and resolving their reading abilities. By doing so, it has enabled those who were “educationally and socially rejected.” In reality, these people were just the “approval deprived,” excluded, looking for somewhere to be approved of by, to belong to. Somewhere that was not in denial of these intelligent, potentially unloved, uncared for, yet inspirational individuals, who were perfectly capable of self-modifying their behaviours but were, for the most part, disabled from reaching their fuller potential, especially those ending up in the revolving door of youth and adult custody.
Hence a paper.
- S. Elliott proposed “In our beginnings are our ends, and in our ends are our beginnings.” that, for far too many of the functionally illiterate is far too true.
This paper is aimed at those curious for a better understanding of the Foundation’s campaigning for improved Digital Literacy rates in the UK and attempts to explain its concerns around 21st Century public eye health.
It is a paper which deliberately zooms out to illuminate the wider picture, to give a better understanding of how current ocular and educational paradigms are working against both children and adults, and which aims to provide an exploration of the current WHO classification and scaling of “asthenopic” disease, and truly show it in its entirety, as if for the first time, and shed light on what that means for society.
Presentees have been identified as being those individuals who, despite suffering fatigue, ill-health and being less able to function efficiently, continue to go to their workplace, spending longer hours at work, yet are significantly less productive.
It seems that there is a chain of causation between childhood / teenage visual disruptions and those suffered by a significant number of display screen users both in education and in the workplace for a majority of operators, who are experiencing early onset debilitating eye-strain, resulting in presenteeism and dysfunction.
This deficit we believe is due to visual disruptions linked to over-exposure to the near or close-up, exacerbated by sub-optimally accessible standard display screen equipment and reflected in the growth of interest in ‘visual ergonomics’ across today’s scientific communities.
In this document we aim to make an educational and business case for compliance with internationally accepted Accessibility Regulations, including the introduction of a reasonably practicable and mitigative solution for objectively optimising the standard display screen colour contrast interface. This will improve ease of accessibility and act as a practical Well-being and visual risk reduction intervention.
- Keywords: Human Factors, Functional Illiteracy, Eye-strain, Computer Vision Syndrome, Screen Fatigue, Stress Related Visual Adaptations, Pre-existing and/or Induced Myopic & Asthenopic Disease in the 21st Century, Accessibility, Literacy, Diversity and Inclusion, Sub-Optimal Digital Screen Interface, AI in Digital & Future Technology.
Is insufficient access to daylight and over exposure to near and close up in early childhood, exacerbated by the prolonged use and/or operation of a standard DSE interface, driving Myopic and Asthenopic Disease in the 21st Century?
Five million adults[1] in the age diverse UK population are functionally illiterate. The UK prison population alone houses 50% of inmates[2] who are considered illiterate, with a reading age of 11 years or lower. 58%[3] of the UK workforce is suffering from exposure related visual discomfort, (eye-strain), and 1 in 3 are suffering with arguably either inherited or induced myopia[4].

The economic impact of this in the UK from the resulting presenteeism is estimated by the ONS to be between £36 – 80 billion per year[5].
Work by Holden et al in 2016 [6] estimates that by 2050, half the world’s population will become myopic, with separate research undertaken in the same year[7] showing that 19%, nearly 1 in 5 teenagers, are currently myopic: a fifty percent increase since the 1960s.
Some, including the WHO are calling this a Global Pandemic.[8]
Our working patterns in 2020 are such that too many of us spend hours in front of a screen, with an HSE meta review of research suggesting that by 2007 58% were already experiencing eye-strain or Screen Fatigue[9] [10] referred to in the UK as well as in the US as Computer Vision Syndrome.[11] This provides a strong rationale for the identification of an additional work-stress, working in conjunction with other stressors. The result? – “Presenteeism” – staying at work despite being unfit for work, fatigued and often remaining for more hours than contracted, but not actually being productive, now accounts for an average 20% lost productivity or 1 day in 5.
It is proposed that 72% of the UK population is at risk of presenting with, or developing, induced visual disruptions, and we live in an increasingly urban indoor world, driven by display screen equipment which is perceived as safe or harmless but which, without intervention, is unintentionally, inadvertently, designed to induce these same disruptions.
How did we get here?
Myopia, also referred to as near-sightedness[12] or short-sightedness, is a condition where objects at a close distance are clear, and in focus, while objects further away appear blurry. Conditions associated with myopia are amblyopia[13] and strabismus[14] know generally as ‘lazy eye’ and ‘cross eyed’.
Myopia is a physiological and/or neurological focusing issue due, in part, to the shape of the eye. The soft orb in childhood may become elongated or foreshortened due to inflammation of the retina, increasing or lessening the distance from the cornea to the retina. This elongation causes light entering the eye to be focused in front or behind the retina instead of on the retina, hence the blurred image[15].
Myopia can be a progressive disorder, and is associated with increased risk of retinal detachment, choroidal degeneration, cataracts, and glaucoma.[16]
Perceived causes of myopia
There are several schools of thought regarding causation, one that myopia is a hereditary condition, another that it is environmental. Currently scientists believe that it could be both[17][18][19]. Research findings suggest that some are more genetically prone to myopia than others, nevertheless environment and increasingly limited time spent outdoors also play significant roles.
A systematic review undertaken in 2015 by Hsui-Mei Huang et al[20] concluded that more time spent on close-up work activities was also associated with a higher risk of myopia, and that developing strategies to reduce the impact of near work was vital to reduce unintentional harm to our visual systems.
Myopia has been well chronicled throughout the ages: Aristotle, in 330 BC documented near-sightedness. Dante (1256-1321) made the first known use of the word Asthenopia for eye-strain, and Johannes Kepler(1571-1630), who is attributed with the idea of using specific lenses for correcting near-sightedness, wrote in his work, ‘Clarification of Ophthalmic Dioptrics’ in 1604, about eye damage among children who did too much close work, and is said to have attributed his own near-sightedness to the amount of reading he did.
Dr Rudolf Virchow in 1869 combed the records of German children who attended compulsory education, finding that top of the list of issues noted was eye damage. He found that the longer the child was in school, the worse the eye damage. In a more recent German study from 2014[21], the findings again showed that near sightedness was linked to more schooling.
(For the purposes of this paper we are defining myopia as an asthenopic stress response to induced visual repetitive stressors resulting in injury or adaptation to over-exposure to the near or close-up visual demands.)
Myopia is only part of the story.
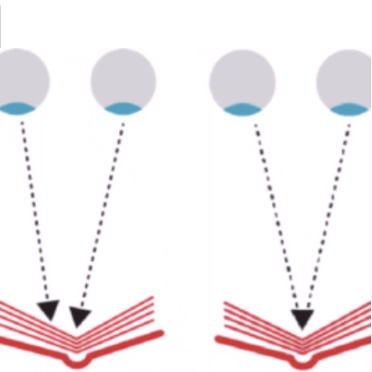
For Binocular Vision (BV) both eyes need to be pointed at and converged on the near target, and then focussed. Muscles outside of the eyes (extra ocular) lock onto the target, whilst the muscles within the eyes maintain focus. Both sets of muscles need sustained stamina to do this but, when fatigued, they are unable to maintain convergence resulting in blurred or worse double vision.
fig: Convergence
BV disorders arise when the eyes target and focus on different places, the brain is then left to process or interpret conflicting images. If it is unable to fuse them together as a single stereoscopic image when faced with these two separate images, the brain compensates by suppressing one image, fully or partially. This is known as suppression or binocular rivalry driving monocular adaptation.
When reading, these issues present as word displacement, reversal of letters and words, shadowing in the spaces between words, or just alphabet soup.
Binocular vision disorder can be a condition present from birth, but can also be caused by injury or trauma to the head, brain damage or stroke and is also well documented as being caused by headaches, anxiety, and other stressors.
Issues related to BV disorder, as with myopia, are amblyopia and strabismus: all are caused by muscle fatigue, an imbalance between eye muscles, or weakness and potential habitual eye-turns designed to reduce the stress of sustaining 3D vision.
A new understanding of BV issues[22] shows that they are possibly the vital component when treating myopia and amblyopia. Stress and accommodative lag (time to focus) are features of myopia, the two may well be intertwined.
Surprisingly, there is no routine test for binocular vision for children in England, but, it is part of the routine testing in Wales, Scotland, and Northern Ireland[23].

An editorial in Optometry and Vision Development in 2010[24] by Dominick M. Maino entitled ‘The Binocular Vision Dysfunction Pandemic’, not only mentions the predicted numbers of adults and children with binocular vision disorders for 2010 but also states that, despite the high number, there is a lack of diagnosis and effective treatment routines, or any national health strategy.
He writes: “a disconnect exists between the high prevalence of BV disorders in the general population and the BV patients reported being evaluated by primary care optometric practices. It’s not that ocular disease is unimportant, it is… but shouldn’t binocular vision anomalies also be diagnosed and treated as well?”
Treatment – Standard Range of Eye Exercises
Eighty percent of learning comes through vision[25] [26]. Small and subtle errors in vision may play hugely damaging roles in this area. American studies have found that numbers of allegedly hyperactive kids were in fact suffering with poor eye teaming[27].
Historically, binocular vision dysfunction has been treated with patching. Records show this being used in the year 900 AD. Patching treats the eyes as two separate mechanical objects, with one that needs strengthening.
Patching as a treatment has many shortcomings; poor compliance and regression being two, yet there has recently been a shift towards vision therapy, where the eyes are treated as working together to form one organ, which works in conjunction with the brain. The aim of the therapy is to strengthen the way the eyes and brain work together.
The primary aim, as suggested by Hess and Thompson (2015)[28] is to ‘restore binocular fusion and stereopsis with an expected secondary consequence of improved vision of the amblyopic eye’.
An excellent example of vision therapy is the use of the Brock String[29].
However, in 2019, the American Academy of Ophthalmology[30] produced a literature review, with no date restrictions, comparing vision therapy to standard patching. 286 citations and 50 articles were reviewed, with 20 articles meeting the criteria.
The findings were mixed, with 2 studies showing huge improvement using binocular vision therapy, yet 5 studies failing to show any improvement over standard patching. The authors do conclude that the more rigorous the research, the less engaging the methods used, so lack of compliance could have played a significant role in the outcomes. As in this often polarised and controversial area, more research is required to turn the anecdotal evidence, of which there is plenty, into quantitative research.
Surgery is another option for correcting strabismus and amblyopia, though this does not always correct the vision, and is often done purely for cosmetic reasons. In 2014 there had been no published research comparing the before and after surgery result in this area for children under the age of seven[31]. A further literature review, this time from 2019[32], highlighted discrepancies in outcome reporting and suggest a consensus among stakeholders, when evaluating strabismus and amblyopia treatments, in what are called Core Outcome Sets.
The role of stress and visual problems.
Ocular issues are stressful to the person experiencing them. There is a range of stress related natural responses linked to “adaptation exhaustion” when attempts to cope with, tolerate or persevere are exhausted, following reasonable alarm. These stress warnings manifest as tiredness, discomfort, fatigue, pain in and around the eye/s, headaches, migraine aura, dizziness, nausea, or worse vomiting, preventing the individual from persisting with close-up tasks especially reading.
With ocular health, these symptoms are reflected time and again as shown in the ICD 10 Index[33] scaling the range of monocular adaptations.
Yet beyond stress – school, lighting, too much screen time, homework and toxic environments and too little time spent outdoors all add to this issue.
In 1996 Merril D Bowan[34] wrote about the effects of stress upon the eyes of children and that stress could change the shapes of the eyes. He was shunned for his opinions that the school environment was stress inducing. His controversial article appeared in the Journal of Behavioural Science, in which he wrote,” the school desk and its reduction of the opportunities for movement is a similar environment to that of the laboratory animal. Containment of a laboratory animal clinically raises the production of ACTH, (Adrenocorticotropic hormone, the hormone that regulates cortisol).” Bowan speculated about the personalities associated with myopia and hyperopes, and suggests that each personality will behave differently, releasing slightly different chemicals in stressful situations, and this could affect the structures of the eyes.
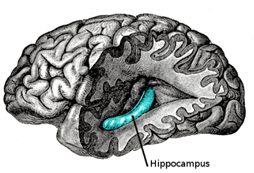
Current data regarding stress and the developing brain, and what are called ACE’s – Adverse Childhood Events, show that stress is an obvious area of research for ocular health. Writing about ACEs’, Maryland Coalition of Families[35] explain that, with trauma, “the hippocampus (the area of the brain that processes emotion and memory and manages stress) shrinks.
ACEs can impact brain development, which in turn impacts functions such as decision-making, self-regulation, fear-processing, memory and stress management.”
The WHO claim stress “can disrupt early brain development and compromise functioning of the nervous and immune systems.”
This leads one to ask the question, if stress can cause epigenic changes to our genes, then is the changing of the shape of the developing hippocampus also a plausible route to explaining the effects on the eyes, as suggested by Bowan?
When trying to understand the challenges for a child reading off and/or on-screen, with or without an ocular issue, author and dyslexic campaigner Ian Jordon[36] describes the difficulties in his book “The circle of Underachievement”. He writes, “All critical information in schoolwork is presented to the child in their central visual areas.
Convergence and accommodation are stretched to their limits, saccadal (jerky) movement is utilized continuously , virtually all the time, instead of pursuit movement. The lights and computer screens flicker at a rate that is disturbing, and the text creates patterns, which are often a direct cause of visual stress. It is surprising that so few have major problems. It is a completely different environment from that to which our visual system is optimally tuned.”
“Reading is a multifaceted process that is influenced by psychological, physiological, environmental, sociological and linguistic factors”, (Christian et all 2017[37]).
The impact of computer technology on public health
In 2017/18[38] statistics show that 88% of UK households owned a home computer: in 1985 it was a mere 13%.
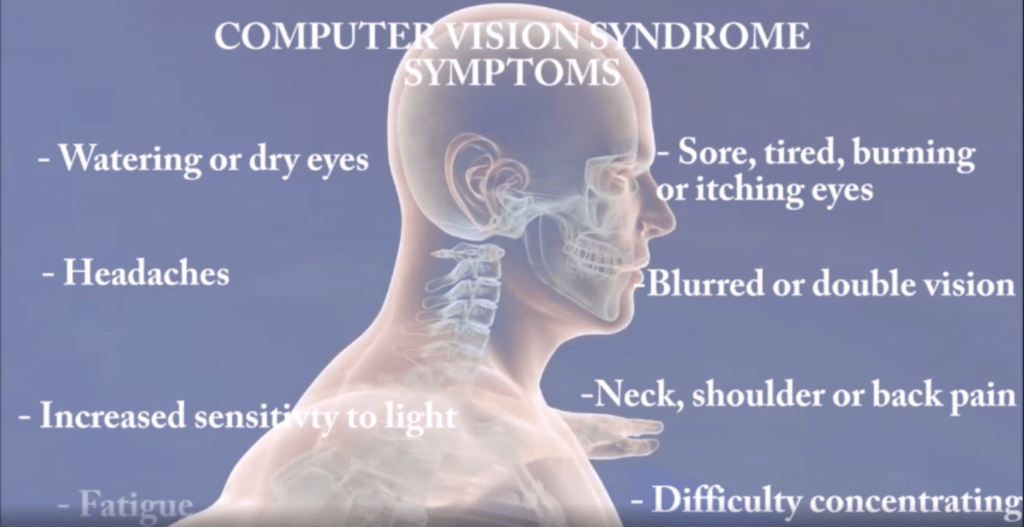
In 2014, Akinbinu and Mashalla [39]published their literature review on the impact of computer technology on health, specifically looking at Computer Vision Syndrome (CVS), symptoms of which are eye strain, burning sensations, blurred vision, and headaches. CVS is aggravated by poor lighting, glare and improper workstation set up.
The paper found that prolonged computer usage, considered as more than 4 hours per day looking at a computer screen, leads to CVS symptoms. Seventy percent of screen users reported issues with their vision.
The American Optometric Association (AOA) define CVS as a complex of eye and vision problems related to activities which stress the near vision, and which are experienced in relation to or during the use of a computer.
Computer work includes frequent saccadic eye movement, accommodation and vergence, all involving continuous muscular activity. This is due to the screen images being made of pixels, which have bright light at their core, becoming darker at the periphery, causing electronic characters to blur around the edges. The blurring of the edges makes it harder for the eyes to focus when looking at a screen. Findings highlighted within the review show that the human eye finds today’s computerised gadgets difficult to cope with. In many cases the symptoms of CVS occur because the visual demands of the task exceed the visual abilities of the individual to comfortably perform the task.

All symptoms of CVS were found to be worse in those who express anxiety, stress, and depression; who work over 5 hours more than contracted, but take no time off, in other words – presentees.
A more recent systematic review[40] published in 2020 looking at the effects of computer screens and myopia, gives mixed findings, with some reports showing an effect, but others not. The summary of the review suggests further research in this area.
Screen time, especially during the 2000’s is a much-discussed topic. We are living in what has been described as an ‘always on culture’, where the lines are blurred between home and work: this is considered detrimental to mental health. A survey published July 2020[41] found that many employees would welcome regulations to manage technology and screen time exposure.
Under the 1999 Management of Health and Safety Regulations, employers have a legal duty to assess and protect workers from work related stress. Screen time may soon be added to the list following campaigns by the NHS and Royal Society for Public Health.
RSPH Campaign Look after your Selfie
But here is where it becomes interesting. Binocular Vision disorders present very similarly to, even mirror those of Computer Vision Syndrome, with symptoms such as headaches, eye strain, blurred vision, and double vision.
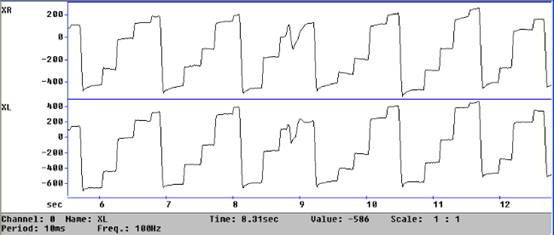
fig: Eye Tracker Trace of Two Eyes Not Able to Track Consistently Together
However, following development of a “Validated Asthenopic Assessment”, we can now differentiate between symptoms linked to Dyslexia and the symptoms predicting visual disruptions presenting in 3D vision loss.
Validated Asthenopic Assessment
Impact & Management of Day / Work lighting in schools and offices

When looking into the effects of lighting in offices, the majority of papers refer to commercial productivity[42].
Those that do look at ocular health[43], find that poor lighting has an effect on degree of fatigue, the eyes and on overall health. Fluorescent lighting and compact fluorescent light bulbs, an energy saving version, are both known to cause eye strain, with symptoms of dry eyes, double vision, headaches, and poor concentration. This is due to their production of an artificial source of ultraviolet (not Blue) light known to cause cataracts and macular degeneration[44].

Health and Safety International in 2012[45] produced an in-depth article related to eye health in the workplace and noted that it wasn’t only the light that needed looking at.
The report highlighted a bullet point list of other factors that impact on the health of the eyes. These include time to focus on an object: fast moving objects are hard to see. Brightness: too much or too little reflected light and insufficient day and/or work lighting – not enough light for the need – making objects hard to see. Mentioned also are poorly distributed and or flickering lights or Doppler effect between lighting and screen, which have been classed as a very real hazard in workplaces today.
When looking at the lighting in schools, the focus tends to be on mood and concentration, academic performance, and alertness. Eye strain is barely mentioned, with one website stating that reading in dim light merely tires the eyes but doesn’t cause lasting damage. However, Dr Richard Hobday PhD, Engineer and author of The Light Solution is convinced that poor lighting in schools is triggering myopia[46].
Writing in Perspective in Public Health, Hobday charts the aetiology of myopia and the changing opinions relating to its causation. Schools a hundred years ago believed poor lighting caused myopia, but in the 1960’s myopia was believed to be genetic and nothing whatsoever to do with lighting or close-up work. Currently, myopia is again being attributed to the school environment and lack of outdoor time. Hobday writes, “At the beginning of the last century, high levels of daylight in classrooms were one of a number of measures thought to prevent myopia, and some eye specialists campaigned for what they referred to as ‘ocular hygiene’ in schools. They stated that children had to learn how to see properly, without straining their eyes, if they were to preserve their eyesight.”
Ophthalmologist Dr Starr[47] from Weill Cornell Medical College agrees with Hobday and feels children should spend much more time outdoors, suggesting an extra 3 hours a day. He explains that dopamine, a vital component in eye growth in children is stimulated by daylight. Dopamine is said to prevent the eyes from elongating, which is, as noted above, a cause of myopic vision.
Indeed, a recent pilot study from China[48] found that schoolchildren and teachers prefer what they call brightly lit classrooms, ones that reflect more natural day light.
Are Regulations or just absence of compliance letting us all down?

In 2017, there was a mere a 10%[49] compliance with UK 1993 Display Screen Regulations (DSE) in the UK accepting that these excluded display screen interface ergonomics or accessibility, trending in the lead-up to 2020.
It can reasonably be argued that this needs to change, and that UK employers need to act on Occupational Health and Accessibility regulations: a precedent has already been set with Baker v Quantum Clothing[50] in 2011. This case dealt retrospectively with work related hearing loss directly linked to a noisy factory environment, it was decided on appeal and held up in the Supreme Court that the employer should have been aware of evidential changes and not solely relied upon current, at that time, Health and Safety working directives so, that ‘reasonable foresight’ was relevant and they should have and aught to have implemented safeguards and were therefore deemed negligent and liable.
Current Regulations:

UK DSE Regulations were first created in 1993 and amended in 2002[51] . However it was noted that that although DSE is written large on the Tin, even in fact, in the title, only furniture and seating were included in risk assessments.
Regardless of continued complaints of discomfort, eye strain and headaches, these were dismissed as temporary, leaving users and operators, including those with existing visual deficits and/or on the Neurodiverse / Dyslexia spectrum, at a 4 to 7 fold significantly increased risk of suffering early onset eye-strain, fatigue, work-stress, presenteeism and repetitive injuries as DSE operators.
Yet we now know that computer glare[52] – both direct and indirect – causes the visual system and muscles of the eyes to overwork. Even the publication of the HSE Better Display Screen RR 561[53] work-related ill-health data in 2007, established that 58% were effectively over-exposed to standard unmitigated calibration of DSE interface, and reported suffering work related eye strain. Commissioned by the HSE the extensive literature review informed the findings of RR561 and ,“showed a significant influence of DSE work, in that the prevalence of symptoms were higher among those who spent more time at their computer at work and among those who worked for longer without a break. All symptoms were more common among respondents who had indications of stress, anxiety and/or depression. “
WCAG 2.1 [54] Is a web content accessibility guideline 2.1 (2018), extending the existing 8878 guidelines published in 2008. Unfortunately these are only recommendations and advisory, based upon four principles: perceivable, operable, understandable, and robust enough to be understood and interpreted by a wide range of professional website designers.
ISO 30071.1 has been developed to reinforce the 1998 PUWER Act (Provision & Use Work Equipment Regulations) assisting the builders of digital products to ensure sufficient adaptability for the 45% of the UK who suffer a disability of some kind, to be enabled to “access” / customise their screen products.
The UK Government 2018 Accessibility Regulations for Public sector[55] websites are to be accessibility compliant by 23rd Sept 2020, but for some reason schools are exempt from the regulations. The public sector accessibility standards, at this time only apply to local government, the police forces, fire and rescue, the NHS and Universities and colleges.
Interestingly it could be that children are not considered users[56], and so are exempt from Health & Safety occupational health protection yet, before, during and post COVID 19, children are as often online as much, if not more than their parents.
We now have a Global population that is visually distressed.
Currently adults and children are doing their best to function with impaired vision, and increasing numbers are exhibiting poor or diminished literacy skills, aggravated by prolonged display screen use, poor or sub-optimal lighting in schools and offices, and poor diagnosis and care of induced visual disruptions. This is initiating or exacerbating the degree of stress, performance anxiety and the range of self-harming comforting or destructive behaviours driven by suppressing or giving reign to the natural fight, flight or freeze responses.
The consequences of the predicted ocular pandemic, that of half the global population experiencing poor vision and poor depth perception, will impact on all areas of life; driving, operating machinery, sports activities, work related tasks and even simple actions such as pouring liquid into a cup[57]. The current costs of this will balloon exponentially, and already the Singaporean Air Force is becoming increasingly alarmed at the rate of myopic trainees. Asian expenditure on laser treatment is skyrocketing as they try to remedy the levels of myopia, with currently [58] 80-90% of children graduating in Southeast Asia being myopic.
Knowing this, what can be done?
Dr Mutti, Professor of Optometry at Ohio State University, in 2010 discussed his then 20-year-long investigation into myopia and concluded that outdoor time and daylight are vital to reduce the incidence of myopia in children, especially in those with myopic parents. He wrote, “If children engaged in over 14 hours per week of outdoor activity, their chances of becoming near-sighted were now only about 20 percent. Quite a dramatic reduction in the risk of becoming myopic.”[59]
We have already referenced the study from China that concluded staff and children prefer brighter classrooms with natural light, and we have referenced and explained issues with school and office lighting. It is up to the governments and employers to modify these issues.
Complicating the matter is that the solutions to ocular health are often highly individual. As Dr Richard Hobday said, “one person’s glare is another’s phototherapy.”
Put simply, better eye care, examination, problem identification and earlier more effective treatments are required, all of which are covered by laws, which are unfortunately underutilised and by and large unknown by the population/Human Resources.
The regulations must be enforced, and additional solutions need to be found. However, the use of colour is once again emerging as a reasonably practicable aid to reduce harm of repetitive stress injuries to the eyes, especially as the hazards of over-exposure to the near or close-up are also known knowns.
The use of intuitive coloured overlays and tinted glasses has been well documented, but what is evolving is the next generation of “subjective coloured display screen interface optimisation”. This new, objective methodology was developed originally as a Digital Literacy aid for teenagers but is now being developed as a Wellbeing Tool for those in education, as well as for DSE operators in the workplace, to mitigate repetitive visual injuries in an age diverse population which is already coping with poor environmental factors, in addition to personal visual issues.
Colour optimisation and visual stress.

The WHO has adopted the term Asthenopia as a heading for the range of monocular adaptations, conditions or diseases, spanning the non-specific symptoms of discomfort and fatigue of the eyes which cause visual distortions.
Visual stress is said to be caused by deficits in sensory input, not by binocular convergence or accommodation, and has also been shown, according to Kriss and Evans (2005[60]), to affect 12-14% of the population and 25% of non – dyslexic children.
Visual stress relief or reading gains have long been seen reported in the use of “coloured overlays” or “tinted-glasses”. This has been a controversial subject with arguably inconclusive evidence to date. The studies so far have included small numbers of participants, and because it is known that the optimal colour is 100% individual, it is difficult to find statistical evidence, especially, if the colour selection is solely subjective or intuitive using a palette of colours.
Once again, we are in a land of plenty of anecdotal evidence, but not enough to convince empirically.
With the application of colour, again we have a timeline; not as long as the one for myopia or BV disorder, but the timeline is there, nonetheless.
Beginning in 1958, JJ Jansky[61] Former Assistant at the Paediatric Language Disorder Clinic in New York, mentioned a student who couldn’t read the words when they were printed on white paper, but could when they were printed on yellow.
In 1980, Olive Meares, a New Zealand teacher described the difficulty some students experienced due to visual distortions when reading black text on white paper.
At around the same time, in 1983, Psychologist Helen Irlen began writing about transparent colour overlays to assist with reading difficulty. Allegedly they were unaware of each other’s work in the 1950’s , but were both describing remarkably similar symptoms, and as such, when the symptoms were discussed, they were often referred to as Meares-Irlen Syndrome.

Coloured overlays and tinted glasses have been widely used for those with dyslexia.[62]
Though this paper does not have the scope to fully discuss this area further, needless to say the topic is polarised amongst the Dyslexia community.
More recently, Professor Arnold Wilkins has contributed hugely to this area of research. He is currently Emeritus Professor of Psychology at the University of Essex and in 1993 was the designer of the Intuitive Colorimeter, a device which allows the reader to quickly identify the best personal colour for tinted glasses for themselves.
Professor Arnold Wilkins describes the theory behind using coloured overlays as that of reducing visual sensory stimulation. In his TED[63] talk he clearly explains how the human brain and eyes were designed for nature. Nature isn’t made up of vast contrasts of colour, straight lines, or stripes. Our modern world is full of them, and it is the stark contrast in colours and stripes that are stressful to the human visual system.
Words and text are presented as a condensed form of contrasting colours, e.g. black on a back-lit white background, which creates striped forms.
Not only do the lines of the written text form stripes, but so do the words.
Wilkins gives the example of the word MUM, made up of vertical stripes. This sensory input can cause overexcitement in the visual cortex, causing cognitive and related visual discomfort which is measured by an increase in oxygen use. The body’s natural response is to turn away from this discomfort. The high oxygen use is a sign of high energy expenditure, which can then lead to fatigue. However, when you are learning to read, or having to read, to turn away is nowadays seen as an inability to focus and concentrate: it is not seen as a natural physiological response.

Coloured overlays dissipate the excessive excitation and lower visual stress. This calms down the central nervous system, and increases ease of access to the text, and thereby reading speed, which is transformed from halting to fluent.
The role colours plays is still not fully understood, and again this doesn’t help move the case forward. If it is that perceptual distortions occur because a spread of excitation already causes visual neurons to fire inappropriately in response to visual stimulus, imagine if you then add myopia, binocular convergence disorders, the fight or flight response and a flickering classroom light?
You would have a child or adult unable, possibly unwilling to read, because the entire experience is incredibly uncomfortable to the central nervous system.
What is needed is an objective method of fine tuning the contrasting screen background colour for the individual, to enable optimal accessibility and performance whilst mitigating eye-strain and predictable risks of further of exacerbating visual injuries or self-harm caused by “carrying-on regardless”.
The next generation of display screen interface optimisation:
Subjective digital display screen interface adaptations are already here. There are extensions in the Chrome browser and others, extensions, for mobile devices and software, which enables you to adjust your personal device screen, but again, they fall short of being a solution because they are intuitive, limited in colour range and cannot be precisely be optimised for the individual, which is the critical component.
The key is finding the very specific contrast colour / hue that calms the excitation, that allows reading on-screen to be a comfortable experience while moving the central nervous system toward the parasympathetic model.
Removing or reducing the levels of discomfort will also reduce the risk levels of visual repetitive stress injuries/adaptations, while at the same, being compliant with legislation. This legislation clearly recognises that colour contrast validation of websites is important, and regulation ISO 30071.1 also recognises that display screen interfaces are intrinsically harmful unless adjusted and/or customised for the specific user operator.
SMART Foundation have developed a unique methodology for the optimisation of the DSE Interface which is relatively seamless, interactive, semi-automated and which, most importantly, achieves a more optimal accuracy versus the current subjective or intuitive “best fit”.
The software is a non-invasive and reasonably practicable method for assessing a subject’s overall stress levels, working as a diagnostic tool, as well as effectively identifying the optimal RGB values for their display screen, thereby offering a therapeutic calibration to reduce this predictable eye-strain, whether it be pre-existing or potentially induced and driven by CVS or Screen Fatigue. In due course, it is anticipated that the software will remove the current need for the user to be interactively required to start and end each scanning of the subject matter in a timely manner, thus removing any potential user inaccuracies affecting the outcome.
It will measure real time fatigue, using AI and biometrics during live screening and record physiological and neurological reactions, to ensure even more accurate RGB contrast values for their display screen text interface.
Anecdotal evidence has grown, as many participants comment that, “they didn’t know they were under so much stress”, experience emotional relief through shedding a tear or two, together with perhaps either relief or even rage, when they realise how easy it is to read when using a display screen interface which has been personally calibrated for them. The profound realisation that they did not know how hard they have had to work previously, simply to access text.
The Proposition
Whilst we may currently have little control over the environment in which screens are used, and certainly have little or no control over exposure to display screens in the office or even over their use by our children, we do know that our modern indoor urban work/life is far from ideal and, regardless of any number of better workplace or health related nudge campaigns, we need to be “solution orientated” rather than just focusing on the identification of visual decremation as being a “problem” versus its being an “opportunity”.
More research is needed to fully position “public ocular health” and well-being on the educational and economic map. It will take time and commitment for regulations to be enforced, for eye examinations to change and improve, and for a new and improved use of day and work lighting in the built environment of our schools and offices. One small change, however, that of display screen interface optimisation, could make a huge difference to prolonging the public’s eye health. It could improve educational and work lives and strengthen the capacity for life-long learning via access to the IOT, e-learning and simultaneously the increasingly SMART digital economy.
The SMART Foundation is therefore looking for both academic and corporate partners to expand the development of the on-line interactive software, and fund further research into public awareness. We wish to be able to use our existing patented software, as a foundation on which to build and develop the next generation of AI driven biometrics screening. Our aim is to eliminate, once and for all, the ambiguity of received knowledge surrounding the health benefits of day light. Finally we want to promote ‘colour as an effective therapeutic treatment’ for pre-existing or induced binocular vision loss.
We passionately believe in the future of AI driven biometrics screening for display screen contrast interface optimisation. We believe it is the way forward to protect the well-being of DSE operators. In the chain of causation, it could offer children with learning difficulties improved access to text and the opportunity to actively participate fully in learning in addition to reducing the overall ocular health burden, both in the UK and Globally.
We shall not cease from exploration
And the end of all our exploring
Will be to arrive where we started
And know the place for the first time.
- S. Elliott
Nigel Dupree
Project Director
S.M.A.R.T. Foundation
[1] Singh A (2019) Millions of British Adults are Functionally Illiterate. The Telegraph. Jan 5th.
[2] Moss S (2017) Half of Britain’s prisoners are functionally illiterate. The Guardian. June 15th.
[3] https://www.hse.gov.uk/research/rrhtm/rr561.htm
[4] https://www.nhs.uk/conditions/short-sightedness/
[5] Will Hazel (2018) Illiteracy Costs UK £36 Billion a Year. tes.com March 23rd.
[6] Holden et al.: Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050, Opthalmology, Volume 124,(3) March 2017, pages e24-e25.
[7] https://www.college-optometrists.org/the-college/media-hub/news-listing/nicer-myopia-children.html
[8] Gonzalez-Meijome.:New Research Routes to Fight Myopia, EBioMedicine, Volume 16, February 2017, pages 24-25.
[9] https://www.huffingtonpost.co.uk/entry/screen-fatigue-working-from-home_uk_5e7a0f5fc5b62f90bc51a264
[10] Sheppard A, Wolffson J.: Digital Eyeye Strain: Prevalence, measurement and amelioration. BMJ Open Opthalmology. Vol3(1) 2018 e000146
[11] Akinbinu TR, Mashalla YJ.: Impact of Computer Technology on Health: Computer Vision Syndrome. Academic Journals, Volume 5(3) November 2014, pp 20-30.
[12] https://www.mayoclinic.org/diseases-conditions/nearsightedness/symptoms-causes/syc-20375556
[13] https://www.nei.nih.gov/learn-about-eye-health/eye-conditions-and-diseases/amblyopia-lazy-eye
[14] https://www.allaboutvision.com/conditions/strabismus.htm
[15] Mayo Clinic Near Sightedness
[16] Smith MJ, Walline JJ.: Controlling Myopia Progression in Children and Adolescents. Adolescent Health Medicien and Therapeutics Volume 6, 2015, pp 133-140.
[17] Vera-Diaz FA.: Myopia. Encyclopaedia of the Eye. 2010 pp 98-105.
[18] Fan, Q., Verhoeven, V., Wojciechowski, R. et al. Meta-analysis of gene–environment-wide association scans accounting for education level identifies additional loci for refractive error. Nat Commun 7, 11008 (2016).
[19] Goldschmidt E, Jacobsen N.: Genetic and Environmental Effects on Myopi Development and Progression, Eye (Lond) Volume 28(2), February 2014, pp 126-133.
[20] Hsiu-Mei Huang, Dolly Shuo-Teh Chang, Pei-Chang Wu.: The Association Between Near Work Activities and Myopia in Children – A Systematic Review and Meta-Analysis. PLoS One. 2015; 10(10): e0140419. Published online 2015 Oct 20.
[21] Mirshahi A et al. Myopia and Level of Education: Results from the Gutenberg Health Study. Opthalmology, Volume 121(10) October 2014, pp 2047-52
[22] https://www.myopiaprofile.com/
[23] https://www.orthoptics.org.uk/patients-and-public/childrens-vision-screening/
[24] Miano DM. The Binocular Vision Dysfunction Pandemic. Optometry and Vision Development, Volume 41, Number 1 , 2010, pp 6-13.
[25] https://www.seyens.com/humans-are-visual-creatures/
[26] https://www.pnas.org/content/95/5/2703.full
[27] https://www.additudemag.com/adhd-and-vision-problems-understanding-symptoms/
[28] Hess RF, Thompson B. Amblyopia and the Binocular Approach to it’s Therapy. Vision Research, Volume 114, September 2015, pp 4-16.
[29] https://youtu.be/EGlCVTdNqfw
[30] Pineles et all.: Binocular Treatment of Amblyopia: A Report by the American Academy of Opthalmology. Opthalmology, Volume 127(2), Februaray 2020, pp 261-272
[31] Korah et al.: Strabismus Surgery Before Versus After Completion of Amblyopia Therapy in Children. Cochrane Database of Systematic Reviews, issue 10, 2014, 15th October.
[32] Al Jabri, S., Kirkham, J. & Rowe, F.J. Development of a core outcome set for amblyopia, strabismus and ocular motility disorders: a review to identify outcome measures. BMC Ophthalmol 19, 47 (2019)
[33] 2020 ICD-10-CM Codes for Visial Disturbances and Blindness (H53-H54)
[34] Merril D. Bowan. New Speculations on Refractive Error. Journal of Behavioural Optometry, Volume 7(5) pp 1996, 115-122.
[35] .” http://www.mdcoalition.org/blog/adverse-childhood-experiences-aces-and-their-impact-on-brain-development
[36] Jordan I. The Circle of Underachievement. 2002, reprinted 7th September 2018. Self-published/Amazon.
[37] Christian et al.: Visual and Binocular Status in Elementary School Children with Reading Problems. Journal of Optometry, Volume 11(3), July-September 2018, pp 160-166.
[38] https://www.statista.com/statistics/274164/pc-penetration-in-the-united-kingdom-uk-since-2009/
[39] Akinbinu TR, Mashalla YJ. Impact of Computer Technology on Health: Computer Vision Syndrome. Volume 5(3), November 2014, pp 20-30.
[40] Lanca C, Saw SM.The association Between Digital Screen Time and Myopia: A Systematic Review. Ophthalmic and Physiological Optics. Volume 40(2), March 2020, pp 216-229.
[41] Workers Back Restrictions on Technology Use. Business Matters Magazine, 14th July 2020.
[42] https://www.cass.city.ac.uk/__data/assets/pdf_file/0004/363217/lighting-work-performance-cass.pdf
[43]Lin KH, Su CC, Chen YY, Chu PC. The Effects of Lighting Problems on Eye Symptoms among Cleanroom Microscope Workers. Int J Environ Res Public Health. Volume 16(1) Jan 1st 2019.
[44] https://americaneyecare.com/is-office-lighting-affecting-your-vision/
[45] https://www.hsimagazine.com/article/lighting-the-way-to-safety-722/
[46] https://www.luxreview.com/2015/03/26/are-schools-ruining-kids-eyes-with-poor-lighting/
[47] https://www.canr.msu.edu/news/the_benefit_of_daylight_for_our_eyesight
[48] https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0181772
[49] https://www.shponline.co.uk/headline-news/dse-compliance-just-10-study-claims/
[50] http://ukscblog.com/case-comment-baker-v-quantum-clothing-group-ltd-ors-2011-uksc-17/
[51] https://www.hse.gov.uk/foi/internalops/ocs/200-299/oc202_1.htm
[52] https://www.news-medical.net/health/Does-looking-at-a-computer-damage-your-eyes.aspx
[53] https://www.hse.gov.uk/research/rrhtm/rr561.htm
[54] https://www.w3.org/WAI/standards-guidelines/wcag/glance/
[55] Abilitynet.org.uk Countdown to 2020 Public Sector Accessibility Regulations Deadline.
[56] http://forum.iosh.co.uk/posts/m639186-DSE-in-Schools
[57] https://opto.ca/health-library/binocular-vision
[58] https://www.plano.co/cloudy-skies-ahead-myopia-against-the-air-force-2/
[59] https://www.npr.org/templates/story/story.php?storyId=122374802&t=1593369279809
[60] Kriss I, Evans B. The Relationship Between Dyslexia and Meares-Irlen Syndrome. Journal of Research in Reading. Volume 28, 1st August, 2005, pp 350-364.
[61] Jansky, J.J. A case of severe dyslexia with aphasic-like symptoms. Bulletin of the Orton Society Volume 8, May 1958, pp 8–11
[62] https://theconversation.com/a-rose-tinted-cure-the-myth-of-coloured-overlays-and-dyslexia-120054
[63] https://www.youtube.com/watch?v=GBOzv9HgoWM&list=LLFokV5rYfyiokrwtbCSn-lw&index=9&t=22s



